Original
Changes in mitral valve position while standing in and out of water
Yuka Ukida1, Takuma Wada2, So Giho1, Yasuo Ishida1, Sho Onodera2
1Graduate School, Kawasaki University of Medical Welfare
2Kawasaki University of Medical Welfare
ABSTRACT
We predict that the position of visceral organs rises due to the decrease of waist circumference of astronauts during exposure to microgravity. Water immersion at the level of the xiphisternum closely simulates a microgravity environment. Therefore, this study aimed to clarify the relationship between the depth of water immersion and heart position. Ten healthy young males volunteered to participate in this study. We measured heart position, heart rate, and blood pressure. Each subject was asked to stand outside of water and in water at varying depths (at the level of the knee, greater trochanter, navel, xiphisternum, and clavicle) for 5 min each. Standing both in and out of water, we measured the position of the mitral valve during the last 15 sec of the 5 min using the ultrasonic diagnostic equipment. We measured the amount of change in the vertical direction and horizontal direction of the heart based on the mitral valve. Using a heart rate monitor, we measured the heart rate after 5 min of rest. Using an Aneroid sphygmomanometer, we measured blood pressure after 5 min of rest. The heart position moved significantly to the left:5 mm at xiphisternum-level water and 15 mm at clavicle-level water compared to that outside of water (p < 0.05). Moreover, there was a significant movement to the posterior:5 mm at xiphisternum-level water and 6 mm at clavicle-level water compared to that outside of water (p < 0.05). A previous study reported that the left lung in healthy young males was slightly smaller than the right lung. Moreover, the heart is found on the side of the left lung. Based on this information, it is likely that the water pressure causes abdominal organs and diaphragm to rise and the heart to move to the left lung. Based on the results of this study, heart position moved significantly to the left in water compared to that of out of water.
(Received:17 April, 2021 Accepted:2 July, 2021)
Key words:Water depth, Standing, Heart position, Heart rate, Blood pressure
I. Introduction
Space is a different environment from Earth because of the microgravity, radiation, and closed environment, affecting astronauts during space missions. Both acute and sustained exposures to microgravity have been reported to affect the vestibular apparatus12), central circulation8), bone1,18), and muscle4,11). Astronauts experience space motion sickness in the initial phase of a space mission because the fluid shift causes blood volume in the heart and brain to increase. This suggests that the change in the position of a visceral organ can be a trigger for stress. Moreover, we predict that the position of visceral organs rises due to the decrease of waist circumference of astronauts during exposure to microgravity5).
It was reported that water immersion at the level of the xiphisternum closely simulates a microgravity environment9). However, buoyancy, water temperature, water pressure, and viscosity also affect the body during immersion.
It was reported that there was a relationship between water depth and venous return, stroke volume, blood pressure, and inferior vena cava15). As the water depth rises, the venous return increases indicating a direct relationship between these two variables15). The cross-sectional area of inferior vena cava, while water immersion at the level of the xiphisternum, is about 185% larger than normal15). The water pressure causes venous return to increase while causing stroke volume and heart rate to decrease15). Moreover, the position of the heart reportedly moves while immersed in water at the level of the neck3). However, only a few reports discuss the direction in which the heart position changes.
Therefore, this study aimed to clarify the relationship between the depth of water immersion and heart position.
II. Method
Ten healthy young males with no history of heart disease (age:21±0.7 years old, stature:172.5±0.7 cm, weight:68.5±7.9 kg, mean±SD) volunteered to participate in this study. The study parameters were as follows:water temperature at 36.2±0.4℃, room temperature at 24.6±1.1℃, and humidity at 78.1±3.8%. All protocols of this study were approved by the ethics board at Kawasaki University of Medical Welfare and conformed to the Declaration of Helsinki (20-067).
We measured heart position, heart rate, and blood pressure. Each subject was asked to stand outside of water and in water at varying depths (at the level of the knee, greater trochanter, navel, xiphisternum, and clavicle) for 5 min each. Figure 1 illustrates the study protocols. Standing both in and out of water, we measured the position of the mitral valve during the last 15 sec of the 5 min using the ultrasonic diagnostic equipment (SonoSite M-Turbo;FUJIFILM). We measured the amount of change in the vertical direction and horizontal direction of the heart based on the mitral valve. The ultrasound examinations were performed with a sector probe P21x/5-1 (FUJIFILM). Gel sonic was used to improve probe-skin contact. The probe was placed at the third or fourth intercostal space at the left sternal border. After mitral valve movement was observed, we drew a mark with a red marker and decided upon the measurement position. The frequency was adjusted to see the entire mitral valve. The mitral valves of all the subjects were measured at the same frequency. We produced movies of the mitral valve movement when it was most clearly seen. Figures 2-1, 2-2, 3-1, and 3-2 show the heart position on dry land and at clavicle-level water. The vertical line in figures 2-1 and 2-2 and the longitudinal line in figures 3-1 and 3-2 shows the attachment of the mitral valve. The arrows in figures 2-2 and 3-2 indicate the direction of the mitral valve movement. We recorded one person’s electrocardiogram with the bipolar induction during a final 20 seconds of 5 minutes rest standing using wireless-telemetric electro-cardiography, water-proof type, (FUKUDADENNSHI Co, Ltd, DS-2202, Japan). We derived average values using the caliper (TOKUSHIMA SEIKI MFG., LTD.). Using a heart rate monitor (H10 sensor;POLAR), we measured the heart rate after 5 min of rest. Using an Aneroid sphygmomanometer (501;KENZMEDICO), we measured blood pressure after 5 min of rest. The data was analyzed using SPSS ver.23.0 for MAC and using one-way ANOVA with repeated measures. Subsequently, the Dunnett’s post-hoc test was used to identify this interaction. P < 0.05 was considered to be statistically significant.
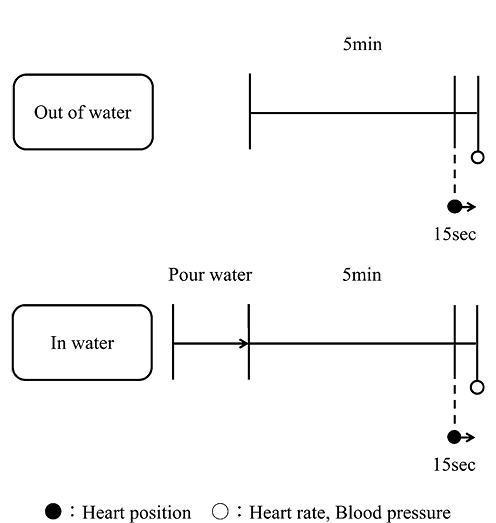
Figure 1 Protocol
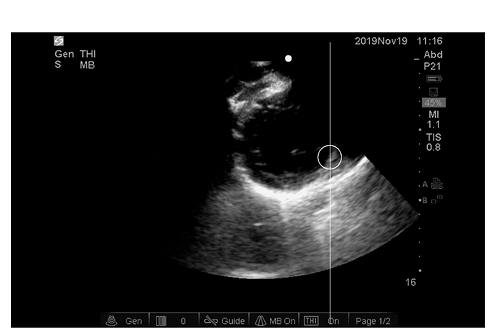
Figure 2-1 Heart position of out of water
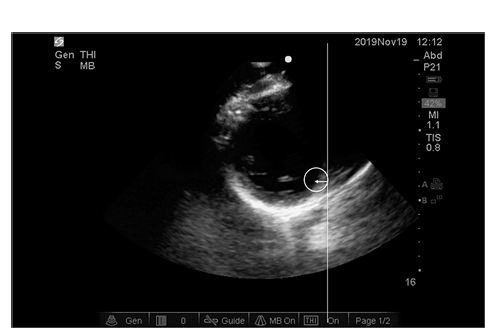
Figure 2-2 Heart position of water depth of the clavicle
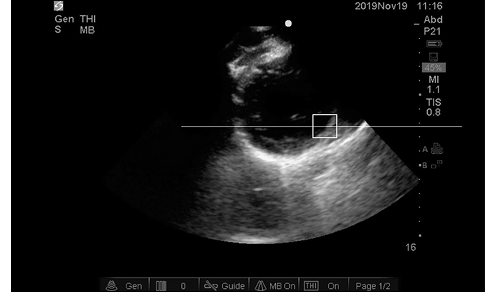
Figure 3-1 Heart position of out of water
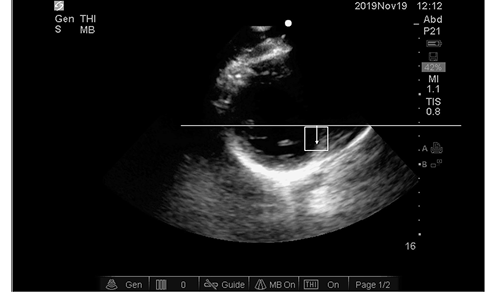
Figure 3-2 Heart position of water depth of the clavicle
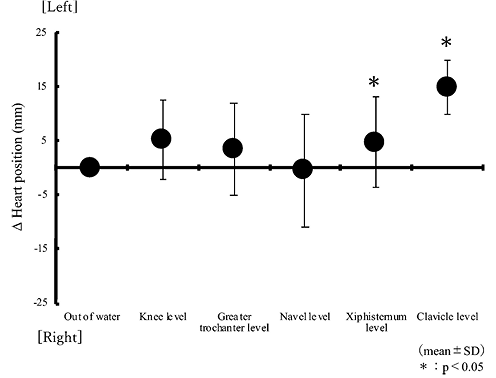
Figure 4-1 Comparison of heart position(Lateral direction)
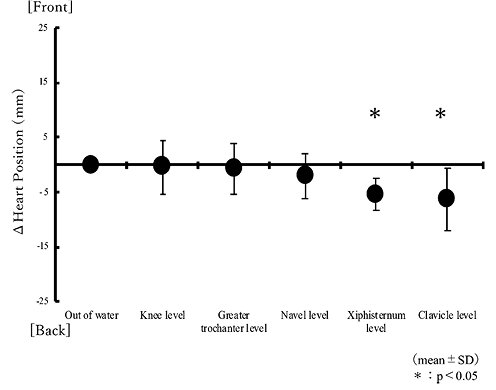
Figure 4-2 Comparison of heart position(anterior-posterior)
III. Results
The heart position moved significantly to the left:5 mm at xiphisternum-level water and 15 mm at clavicle-level water compared to that outside of water (p < 0.05). Moreover, there was a significant movement to the posterior:5 mm at xiphisternum-level water and 6 mm at clavicle-level water compared to that outside of water (p < 0.05).
In the electrocardiogram waveform, the T wave duration was 0.24 s on land, 0.29 1 s at xiphisternum-level water, and 0.26 s at clavicle-level water. The ST segment lasted 0.02 s on land, 0.04 s at xiphisternum-level water, and 0.06 s at clavicle-level water. The QT interval was 0.34 s on land, 0.40 s at xiphisternum-level water, and 0.40 s at clavicle-level water. The RR interval was 0.74 s on land, 0.92 s at xiphisternum-level water, and 0.92 s at clavicle-level water. The T wave for xiphisternum- and clavicle-level water, the ST segment for clavicle-level water, the QT interval at xiphisternum- and clavicle-level water, and the RR interval at xiphisternum- and clavicle-level water were significantly extended compared to those outside of water (p < 0.05). The P wave did not change under the three conditions.
Figure 5 shows the changes in the heart rate, which significantly decreased from 74 bpm (outside of water) to 68 bpm (xiphisternum-level water) and 67 bpm (clavicle-level water) (p < 0.05).
Figure 6 shows changes in blood pressure. The systolic blood pressure (SBP) significantly decreased from 115 mmHg (outside of water) to 110 mmHg (greater trochanter-level water) and 107 mmHg (clavicle-level water) (p < 0.05). Conversely, the diastolic blood pressure (DBP) did not change at any level of water compared to that outside of water.
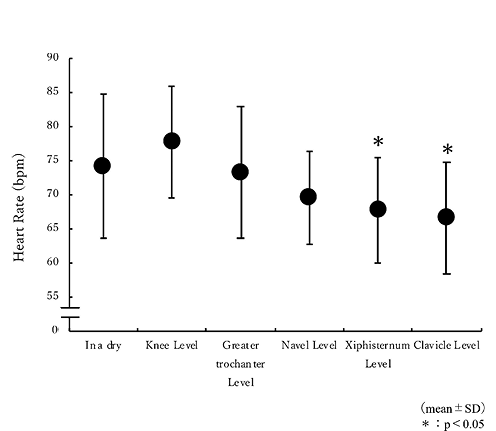
Figure 5 Comparison of heart rate out of water and in water
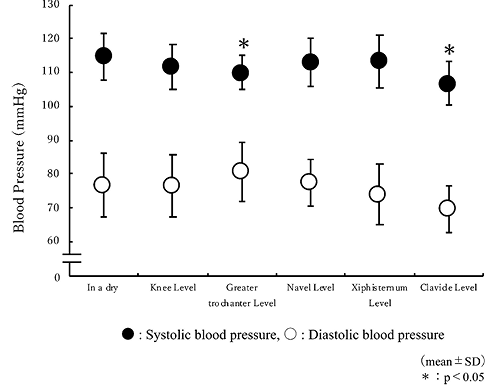
Figure 6 Comparison of blood pressure out of water and in water
IV. Discussion
The findings of this study suggest that the heart position changes even in microgravity, and we observed that the heart significantly changed position to the left and back.
A previous study reported that the left lung in healthy young males was slightly smaller than the right lung6). Moreover, the left ventricle is larger than the right one, and, the heart is found on the side of the left lung. The waist circumference in water is significantly reduced compared to that of out of water3). Similarly, the waist circumference of astronauts decreases during exposure to microgravity5). Displacement of the viscera is observed into the thorax, increasing gastric pressure, and the pressure and gradient across the diaphragm, thereby stretching the diaphragm10). Based on this information, it is likely that the water pressure causes abdominal organs and diaphragm to rise and the heart to move to the left lung. We consider that the same phenomenon is observed in space as well. We expect that water pressure will cause the diaphragm to rise and tidal volume to drop, and that a similar phenomenon will occur in microgravity.
From the results of the electrocardiogram, we considered that clavicle-level water, which is above the position of the heart, prolonged the period of excitement for the entire ventricle7). In this study, it was not possible to determine the QRS complex and transitional zone because we used the bipolar lead. If the displacement of the heart while standing at the depth of the clavicle is pushed up by the diaphragm and simply displaced to the left, we considered that lead I is extended, leads II, III, aVF are shortened, and the QRS axis is near 0°7). From the results of this study, the position at the water level of clavicle was changed to the left and the rear of the body. Thus, on the transitional zone, three thing were assumed. First, V1〜V3 form r waves and V5〜V6 make q waves because the initial excitement of the ventricles faces down7), second, V1〜V3 form S waves and V4〜V6 form R waves because the main excitement waves go to the left7), third, the R wave is the highest at V6 because the apex of the heart points to the left7). In the future, we need to investigate using the 12-lead method to changes in the heart position.
The bladder neck position at pelvic strain was low at supine, sitting, and standing postures14). We consider that the internal organs are affected by gravity. However, there are few reports that discuss the effect of buoyancy on internal organs.
The venous return depends on water depth as well15). As the water level rises, the venous return increases, indicating a direct relationship between the two variables15). The cross-sectional area of inferior vena cava, while immersed in water up to the xiphisternum, is about 185% larger than normal15). The water pressure causes an increase in venous return and an expansion in the left atrial dimension13), causing the heart base to slant posteriorly. Therefore, we can conclude that the heart was displaced to the left when immersed at xiphisternum- and clavicle-level water.
Figure 7-1 shows the correlation between water depth and the horizontal displacement of the mitral valve. The position of mitral valve significantly moved to left in water at the depth of the clavicle. Figure 7-2 shows the correlation between the water depth and horizontal displacement of the mitral valve. From these, we can consider that the heart was displaced posteriorly and to the left in water at the depth of the xiphisternum.
Heart rate in water at the depth of the xiphisternum and clavicle were significantly decreased compared to that of out of water as well (p < 0.05). The water pressure causes venous return to increase and stroke volume and heart rate to decrease, and these variables depend on the water depth15).
SBP decreased significantly in water at the depth of the greater trochanter and clavicle. In contrast, DBP did not change at any level of water compared to that outside of water. During neutral temperature immersion, both SBP and DBP significantly decreased 5 min after immersion2). 5 min after immersion, both SBP and DBP decreased as well16). DBP 5 min after immersion significantly decreased temporarily compared to out of water17) et al., results don’t match. Therefore, blood pressure changes can vary depending on the conditions of immersion.
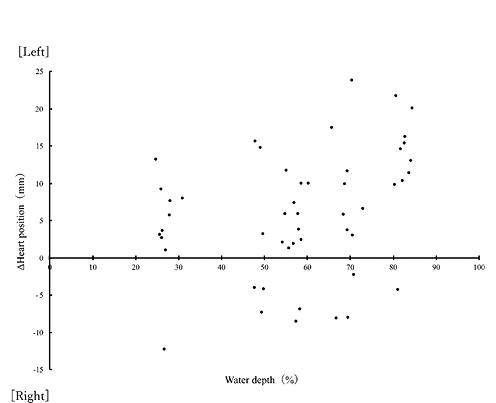
Figure 7-1 Correlation of heart position between water depth(Lateral direction)
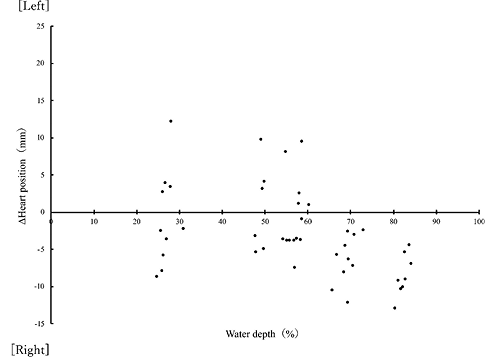
Figure 7-2 Correlation of heart position between water depth(anterior-posterior)
V. Conclusion
Based on the results of this study, heart position moved significantly to the left in water compared to that of out of water.
VI. Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
VII. Acknowledgments
Our sincere thanks to Ms. Ayumi Akiyama, Mr. Daiki Sato, and Mr. Tomoya Shogata for their cooperation in this experiment. The authors gratefully acknowledge Senior Lecturer Tsukasa Tobaru (Kawasaki University of Medical Welfare) for advice on this research.
REFERENCES
| 1) |
LeBlanc, A., Schneider, V., Shackelford, L., West, S., Oganov, V., Bakulin, A. and Voronin, L.:Bone mineral and lean tissue loss after long duration space flight. J. Musculoskel Neuron Interact, 1(2), 157-160, 2000.
|
| 2) |
Sudo, A., Akasaki, F., Yagi, Y., Ijiri, K., Komiya, S., Tsunoda, N. and Watanabe, T.:Effects of the water pressure for the blood pressure in water immersion. JSPEHSS, 22, 51-58, 2003. (In Japanese)
|
| 3) |
Ide, H., Akita, K., Fujiya, S., Asanuma, Y., Agishi, Y. and Morizaki, M.:Effects of Hydrostatic Pressure on Cardiac Function in Human. Hokkaido J. Med. Sci., 62(1), 68-73, 1987. (In Japanese)
|
| 4) |
Akima, H., Kawakami, Y., Kubo, K., Sekiguchi, C., Ohshima, H., Miyamoto, A. and Fukunaga, T.:Effect of short-duration spaceflight on thigh and leg muscle volume. Medicine & Science in Sports & Exercise, 32(10), 1743-1747, 2000.
|
| 5) |
https://iss.jaxa.jp/iss/jaxa_exp/furukawa/exp2/igaku/
|
| 6) |
Tsai, J.Z., Chang, M.L., Yang, J.Y., Kuo, D., Lin, C.H. and Kuo, C.D.:Left-Right Asymmetry in Spectral Characteristic of Lung Sounds Detected Using a Dual-Channel Auscultation System in Healthy Young Adults. Sensors, 17(6), 1323-1334, 2017.
|
| 7) |
Japan Medical Association, Goto, Y. and Obayashi, K.:ABC of electrocardiogram, KYOWAKIKAKU, Japan, 1991. (In Japanese)
|
| 8) |
Otsuka, K., Cornelissen, G., Furukawa, S., Kubo, Y., Hayashi, M., Shibata, K., Mizuno, K., Aiba, T., Ohshima, H. and Mukai, C.:Long-term exposure to space’s microgravity alters the time structure of heart rate variability of astronauts. Heliyon, 2(12), 1-31, 2016.
|
| 9) |
Nishimura, M. and Onodera, S.:Relaxative Effects of Supine Floating on Heart Rate, Blood Pressure and Cardiac Autonomic Nervous System Activity. Japanese Journal of Aerospace and Environmental Medicine, 37(3), 49-56, 2000. (In Japanese)
|
| 10) |
Reid, M.B., Loring, S.H., Banzett, R.B. and Mead, J.: Passive mechanics of upright human chest wall during immersion from hips to neck. Journal of Applied Physiology, 60(5), 1561-1570, 1986.
|
| 11) |
Greenisen, M.C., Hayes, J.C., Siconolfi, S.F. and Alan, D.:Functional Performance Evaluation. NTRS.
|
| 12) |
Reason, J.T.:Motion sickness adaptation:a neural mismatch model. Journal of the Royal Society of Medicine, 71, 819-829, 1978.
|
| 13) |
Masaki, R., Kanaya, S., Morita, S., Migita, T., Hotta, N., Ogaki, T., Fujishima, K., Maruyama, T., Kaji, Y. and Fujino, T.:The Effect of Water Immersion on the Cardiovascular Responses in Healthy Adults in a Warmed Pool─An Echocardiographic Study Using the Pulsed Doppler Method─. J. Health Sci., Institute of Health Science, Kyushu University, Kyushu, 109-114, 1995. (In Japanese)
|
| 14) |
Nishinomiya, S., Morikawa, S., Endo, Y., Masaki, K., Saito, Y., Tsuchikawa, S., Mori, M. and Okayama, H.:The influence of posture on elevation of pelvic organ position. Journal of Shiga University of Medical Science, 26(1), 17-22, 2013. (In Japanese)
|
| 15) |
Onodera, S., Miyachi, M., Nishimura, M., Yamamoto, K., Yamaguchi, H., Takahashi, K., In, Y.J., Amaoka, H., Yoshioka, A., Matsui, T. and Hara, H.:Effects of water depth on abdominals aorta and inferior vena cava during standing in water. Journal of Gravitational Physiology, 8(1), 59-60, 2001.
|
| 16) |
Kishino, T. and Matsuda, M.:Effects of a short time water immersion at subaxillary depth on cardiac autonomic nerve activity─a study in water at 25℃, 30℃ and 34℃─. Japanese J. Phys. Fit. Sports Med., 46, 101-112, 1997. (In Japanese)
|
| 17) |
Kishino, T. and Matsuda, M.:Effects of Short time Water Immersion at the Temperature of 27℃, 34℃ and 38℃ on Cardiac Autonomic Nerve Activity─A study considering the effect of respiration─. BCPM, 61(3), 148-156, 1998. (In Japanese)
|
| 18) |
Lang, T., LeBlanc, A., Evans, H., Lu, Y., Genant, H. and Yu, A.:Cortical and Trabecular Bone Mineral Loss from the Spine and Hip in Long-Duration Spaceflight. Journal of Bone and Mineral Research, 19(6), 1006-1012, 2004.
|
Corresponding author:Yuka Ukida
Graduate School, Kawasaki University of Medical Welfare
TEL:086-462-1111
FAX:086-462-1193
E-mail:wd220001@kwmw.jp